Abstract
Background: Cardiovascular diseases remain the leading cause of morbidity and mortality worldwide. Racial and ethnic minority groups and individuals living in rural areas experience a disproportionate burden of cardiovascular diseases and associated risk factors. Disparities in early detection and management of cardiovascular diseases are driven by interacting social, structural, and health system determinants, with particularly adverse effects among minority populations in both urban and rural settings.
Objective: To systematically review evidence on disparities in the early detection and management of cardiovascular disease among racial and ethnic minority populations across urban and rural settings, identify determinants contributing to these disparities, and synthesize policy and clinical strategies to reduce inequities.
Methods: A structured search of PubMed, Embase, Web of Science, and Scopus was conducted for the period from January 2000 through October 2025. Eligible studies included observational studies, clinical trials, and reviews that examined early detection of cardiovascular diseases and major cardiometabolic risk factors, including hypertension, diabetes, dyslipidemia, obesity, and smoking, as well as management of established cardiovascular diseases among racial and ethnic minority populations. Included studies explicitly considered urban residence, rural residence, and geographic access to health care. Study selection prioritized population-based cohorts, national surveys, and high-quality reviews. Given heterogeneity in outcomes and measurement approaches, findings were synthesized using a qualitative approach rather than a quantitative meta-analysis.
Results: The literature indicates higher incidence and mortality of cardiovascular disease and poorer intermediate risk factor control among racial and ethnic minority populations, including Black populations, Hispanic and Latino populations, American Indian and Alaska Native populations, and South Asian populations, compared with majority populations. Minority populations exhibit lower rates of guideline-recommended primary prevention, including statin therapy, antihypertensive treatment, and smoking cessation interventions, even when clinical eligibility is present. Rural residents, especially individuals from minority backgrounds, experience a higher prevalence of hypertension, diabetes, obesity, and smoking, along with higher cardiovascular disease mortality than urban residents. These disparities are largely explained by social determinants such as income, educational attainment, food access, and health insurance coverage. Inequities in early detection include lower rates of preventive cardiovascular screening, reduced use of cardiovascular risk assessment, and delayed diagnosis of risk factors among minority populations and rural populations. Disparities in management include underuse of evidence-based therapies, delayed treatment intensity during acute cardiovascular events, lower referral rates and participation rates in cardiac rehabilitation programs, and poorer long-term risk factor control. Social determinants of health, including structural racism, neighborhood deprivation, limited access to health care services, transportation barriers, and inadequate digital connectivity, are central drivers of these disparities. Home-based cardiac rehabilitation, tele-rehabilitation, and hybrid rehabilitation models have demonstrated encouraging improvements in participation among patients facing transportation and geographic barriers. Expanding insurance coverage for these services may further improve long-term cardiovascular outcomes while reducing disparities in secondary prevention.
Conclusions: Racial and ethnic minority populations and rural communities experience systematic disadvantages in the early detection and management of cardiovascular diseases. Evidence indicates that interventions integrating policy-level reforms, health system redesign, and culturally tailored community strategies offer substantial potential to reduce these inequities. Future research should prioritize standardized equity-focused metrics, intersectional analyses incorporating race, ethnicity, and geographic context, and implementation science methods to evaluate and scale equitable cardiovascular disease prevention and care models.
Keywords: cardiovascular disease, health disparities, racial and ethnic minorities, rural health, urban health, early detection, primary prevention, health equity.
Introduction
Burden of Cardiovascular Disease Across Populations
Cardiovascular disease constitutes a leading contributor to mortality and long-term disability across global and national populations (Minhas et al., 2024; Muncan, 2018). Advances in prevention, diagnosis, and treatment have reduced cardiovascular mortality in many regions, particularly in high-income countries (Anand et al., 2025). However, these improvements have not been experienced uniformly. Substantial variation persists across population groups, with marked differences observed by race, ethnicity, socioeconomic position, and geographic residence (Javed et al., 2022; Nair et al., 2024; James et al., 2017). These unequal patterns reflect enduring gaps in prevention and care that continue to shape cardiovascular outcomes (Brandt et al., 2023).
Racial and ethnic minority populations and individuals residing in rural communities face a disproportionate share of cardiovascular disease burden (Minhas et al., 2024; Hutchinson and Shin, 2014; Aggarwal et al., 2021). Higher rates of disease onset, greater severity at presentation, and poorer outcomes following clinical events are frequently observed among these groups (Muncan, 2018; Liu et al., 2025; Chaganty et al., 2023). Such disparities contribute to avoidable morbidity, premature mortality, and widening health inequities (Bazoukis et al., 2025; Brandt et al., 2023). Recent global estimates indicate that cardiovascular disease accounts for nearly one-third of all deaths worldwide, with an increasing proportion of disease burden attributable to preventable risk factors. Persistent disparities in cardiovascular outcomes highlight the need for prevention strategies that address both clinical risk factors and the broader social and environmental conditions influencing cardiovascular health. Population aging, urbanization, and changing lifestyle patterns continue to contribute to the rising prevalence of cardiovascular disease in many regions.
Cardiovascular Inequities Among Racial and Ethnic Minority Populations
Evidence from epidemiologic studies consistently demonstrates elevated cardiovascular risk among several racial and ethnic minority populations (Minhas et al., 2024; Muncan, 2018; Javed et al., 2022; Nair et al., 2024). Non-Hispanic Black populations experience earlier onset and greater severity of hypertension, stroke, and heart failure, along with higher cardiovascular mortality (Minhas et al., 2024; Muncan, 2018; Aggarwal et al., 2021). American Indian and Alaska Native populations show a high prevalence of diabetes and cardiometabolic risk factors that accelerate cardiovascular disease progression (Hutchinson and Shin, 2014; James et al., 2017). South Asian populations exhibit increased susceptibility to premature coronary disease, often at lower body mass index levels (Nair et al., 2024; Anand et al., 2025). Many Hispanic and Latino populations carry a substantial burden of obesity and diabetes that contributes to long-term cardiovascular risk (Muncan, 2018; Minhas et al., 2024).
These patterns cannot be attributed solely to individual-level behaviors. Structural factors, including historical and contemporary forms of discrimination, unequal distribution of resources, chronic exposure to psychosocial stress, and persistent inequities within health care systems, play a central role in shaping cardiovascular risk among minority populations (Javed et al., 2022; Bazoukis et al., 2025; Brandt et al., 2023). Differences in access to high-quality preventive services and continuity of care further amplify these inequities (Ali et al., 2024; Faloye et al., 2024).
Geographic Context and Cardiovascular Risk
Place of residence is increasingly recognized as a powerful determinant of cardiovascular health (Bazoukis et al., 2025; Brandt et al., 2023). Rural communities experience a higher prevalence of cardiovascular risk factors, poorer disease control, and higher mortality compared with urban communities (Aggarwal et al., 2021; Liu et al., 2025; Chaganty et al., 2023). Progress in reducing cardiovascular mortality has been slower in rural areas, with some regions showing little improvement over time (Aggarwal et al., 2021; James et al., 2017).
Limited availability of primary care, reduced access to specialty cardiovascular services, longer travel distances, and constrained availability of rehabilitation services contribute to delayed diagnosis and suboptimal management in rural settings (Peterson et al., 2023; Van Iterson et al., 2023; Lipid Association, 2021–2022). Barriers related to transportation, workforce shortages, and limited digital infrastructure further restrict access to preventive and follow-up care (American Heart Association, 2023; NIH/AHA, 2025).
For individuals from racial and ethnic minority populations living in rural areas, these challenges are compounded. The convergence of social disadvantage, geographic isolation, and reduced health system capacity creates conditions that heighten cardiovascular risk and worsen outcomes (Aggarwal et al., 2021; Bazoukis et al., 2025; Health Policy Today, 2025).
Importance of Early Detection and Equitable Management
Timely identification of cardiovascular disease and its modifiable risk factors is essential for effective prevention (Minhas et al., 2024; Anand et al., 2025). Screening for elevated blood pressure, abnormal glucose metabolism, and lipid disorders enables early intervention that can prevent disease progression and reduce adverse events (Benjasirisan et al., 2024; Ali et al., 2024). Equitable management following diagnosis is equally critical for improving long-term outcomes (Faloye et al., 2024; Brandt et al., 2023).
Despite the availability of evidence-based interventions, gaps remain in who receives preventive screening, who is diagnosed at earlier stages, and who receives guideline-consistent treatment (Benjasirisan et al., 2024; Lu et al., 2023). Racial and ethnic minority populations frequently experience delays in diagnosis and lower intensity of preventive therapy despite elevated risk (Ali et al., 2024; Faloye et al., 2024). Rural populations similarly face reduced access to preventive services and ongoing management, resulting in poorer risk factor control (Peterson et al., 2023; Liu et al., 2023).
Purpose of This Review
This systematic review examines disparities in early detection and management of cardiovascular disease among racial and ethnic minority populations within urban and rural contexts. By integrating evidence across clinical, social, and geographic dimensions, the review aims to identify drivers of inequity and highlight strategies with potential to improve equity in cardiovascular prevention and care (Anand et al., 2025; Brandt et al., 2023).
Methods
Study Design
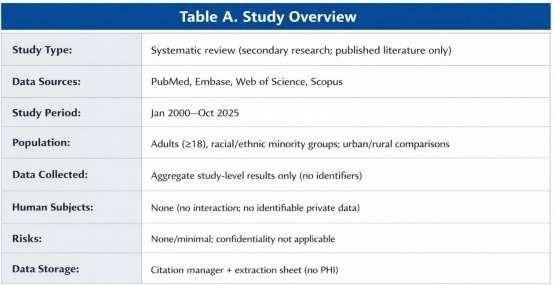
This study employed a structured systematic review approach to examine disparities in the early detection and management of cardiovascular disease. The review focused on synthesizing evidence related to racial and ethnic minority populations and geographic context. Due to substantial variation in study designs, outcome definitions, and analytic methods across the literature, a qualitative synthesis approach was selected to allow comprehensive integration and interpretation of findings across diverse sources (Peterson et al., 2023; Chaganty et al., 2023). The review was conducted in accordance with PRISMA reporting principles for systematic reviews. An overview of the study design and data sources is provided in Table A.
Data Sources and Literature Search
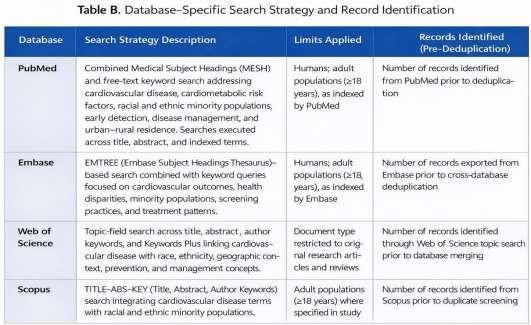
A comprehensive literature search was conducted using PubMed, Embase, Web of Science, and Scopus. The search covered publications from January 2000 through October 2025. Search strategies incorporated controlled vocabulary terms and free text keywords related to cardiovascular disease conditions, cardiometabolic risk factors, health disparities, race and ethnicity, minority populations, geographic residence, preventive screening, early detection, treatment patterns, and long-term disease management (Minhas et al., 2024; Muncan, 2018; Ali et al., 2024).
To ensure completeness, reference lists of influential studies, clinical guidelines, and major statements addressing cardiovascular disparities, rural health, and social determinants of health were reviewed manually (American Heart Association, 2023; NIH/AHA, 2025). This approach helped identify additional relevant studies not captured through database searches alone. The database-specific search strategy and record identification process are summarized in Table B.
Eligibility Criteria
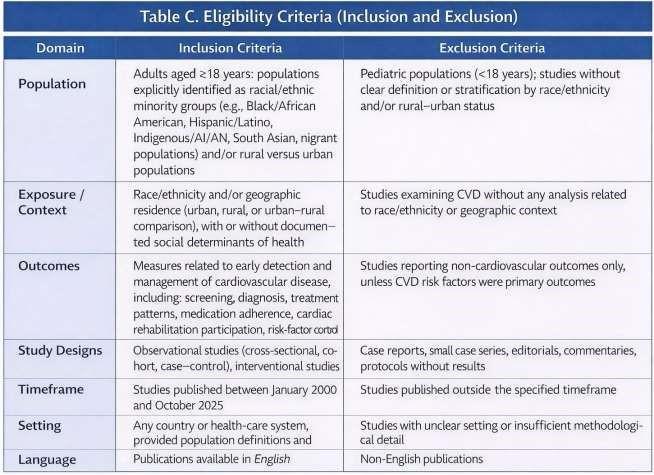
Studies were considered eligible if they focused on adult populations aged eighteen years and older with established cardiovascular disease or elevated risk of cardiovascular disease (Minhas et al., 2024; Muncan, 2018; Anand et al., 2025). Eligible populations included racial and ethnic minority groups, populations residing in rural settings, and populations for which cardiovascular outcomes were reported according to geographic residence (Javed et al., 2022; Hutchinson and Shin, 2014; Aggarwal et al., 2021; James et al., 2017). Urban and rural classification was defined according to the definitions used in the original studies (Peterson et al., 2023; Chaganty et al., 2023). Restricting eligibility to studies with clearly reported cardiovascular outcomes improved the overall quality and comparability of the evidence. Excluding studies lacking adequate methodological detail also reduced the potential influence of reporting bias.
Eligible exposures included race, ethnicity, geographic residence, and related social determinants influencing access to care and health outcomes (Javed et al., 2022; Bazoukis et al., 2025; Brandt et al., 2023). Outcomes of interest included measures of early detection such as screening frequency, diagnostic awareness, and stage at diagnosis, as well as measures of disease management including treatment initiation, medication use, adherence, participation in cardiac rehabilitation, control of risk factors, and cardiovascular morbidity and mortality (Ali et al., 2024; Lu et al., 2023; Benjasirisan et al., 2024; Faloye et al., 2024; Van Iterson et al., 2023; Liu et al., 2023). Eligible study designs included observational studies, interventional studies, and evidence syntheses that provided original quantitative findings and rigorous summaries of primary evidence (Anand et al., 2025; Peterson et al., 2023). Studies conducted in any national context were eligible, provided that definitions of race, ethnicity, and geographic residence were clearly described (James et al., 2017; Hutchinson and Shin, 2014).
Studies were excluded if they focused exclusively on pediatric populations, consisted solely of individual case reports and very small case series, lacked analysis stratified by race, ethnicity, geographic residence, addressed outcomes unrelated to cardiovascular disease, or cardiovascular risk (Minhas et al., 2024; Anand et al., 2025). Detailed inclusion and exclusion criteria are presented in Table C.
Study Selection and Quality Assessment
Titles and abstracts were independently screened by two reviewers using predefined eligibility criteria. Full texts of potentially relevant articles were subsequently reviewed for inclusion. Disagreements were resolved through discussion and consensus. Methodological quality and risk of bias were assessed using study design-appropriate appraisal tools, including standardized checklists for observational studies and reviews (Anand et al., 2025; Peterson et al., 2023). Quality assessments informed the interpretation of findings but were not used as exclusion criteria.
Data Extraction and Analytical Approach
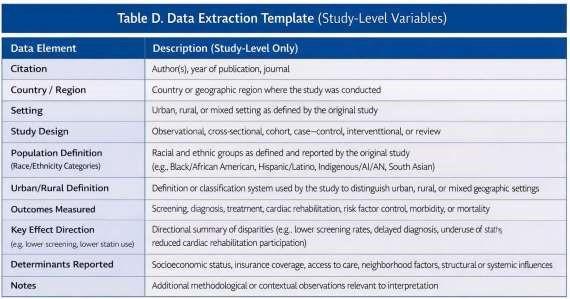
For each eligible study, information was systematically extracted regarding country and setting, study population characteristics, definitions of minority status and geographic residence, and key outcome measures (James et al., 2017; Hutchinson and Shin, 2014). Extracted data related to early detection included screening rates for blood pressure, lipid levels, and glucose levels, utilization of cardiovascular risk assessment tools, and prevalence of undiagnosed cardiometabolic conditions (Benjasirisan et al., 2024; Ali et al., 2024). Extracted data related to management included use of preventive medications, pharmacologic treatment intensity, participation in cardiac rehabilitation programs, utilization of cardiovascular procedures, achievement of risk factor targets, and reported cardiovascular outcomes (Faloye et al., 2024; Lu et al., 2023; Van Iterson et al., 2023; Liu et al., 2023). Review articles were used to identify additional primary studies and to contextualize findings, while synthesis emphasized primary empirical studies to minimize overlap (Muncan, 2018; Anand et al., 2025). Reported drivers of disparities were also extracted, including socioeconomic conditions, health system barriers, structural factors, and measures related to social determinants of health (Javed et al., 2022; Bazoukis et al., 2025; Brandt et al., 2023). Given variability in outcome definitions and measurement approaches, results were organized into thematic domains that reflected burden of disease, early detection practices, management patterns, structural influences, and intervention strategies (Chaganty et al., 2023; Peterson et al., 2023). Emphasis was placed on evidence derived from large national surveys, population-based cohort studies, and methodologically rigorous reviews (Aggarwal et al., 2021; Liu et al., 2025; James et al., 2017). Standardized data extraction procedures improved consistency across studies and minimized transcription errors. Thematic synthesis enabled identification of recurring patterns in cardiovascular disparities while accommodating substantial heterogeneity in study populations, outcome definitions, and healthcare settings. This analytical approach also facilitated comparison of structural, socioeconomic, and healthcare system factors contributing to inequities across different geographic regions. The data extraction framework used in this review is provided in Table D.
Results
Burden of Cardiovascular Disease and Risk Factors in Minority and Rural Populations
Across many included cohort studies and national surveys, cardiovascular disease burden was higher among racial and ethnic minority populations and among rural communities compared with majority populations and urban communities (Minhas et al., 2024; Muncan, 2018; Anand et al., 2025; Aggarwal et al., 2021; Liu et al., 2025). Large population-based cohort studies and national surveillance data demonstrated higher incidence, prevalence, and mortality of cardiovascular disease among multiple minority groups (Minhas et al., 2024; Muncan, 2018; Nair et al., 2024; Hutchinson and Shin, 2014). These differences were observed across coronary heart disease, cerebrovascular disease, and heart failure outcomes (Aggarwal et al., 2021; Chaganty et al., 2023).
Among Black populations, cardiovascular mortality remained disproportionately high and was associated with earlier onset and greater severity of hypertension, heart failure, and stroke (Minhas et al., 2024; Muncan, 2018; Aggarwal et al., 2021). American Indian and Alaska Native populations demonstrated high prevalence of diabetes, obesity, and metabolic abnormalities that were strongly associated with elevated cardiovascular morbidity and mortality (Hutchinson and Shin, 2014; James et al., 2017). South Asian populations living in high-income settings exhibited increased susceptibility to premature coronary disease, often presenting at younger ages with advanced cardiometabolic risk profiles (Nair et al., 2024; Anand et al., 2025). Hispanic populations showed substantial heterogeneity in cardiovascular risk, with several subgroups experiencing elevated cardiometabolic burden and adverse outcomes despite lower aggregate mortality in selected analyses (Muncan, 2018; Minhas et al., 2024).
Geographic context further influenced cardiovascular disease burden. Rural populations experienced higher prevalence of hypertension, diabetes, obesity, and tobacco use, along with persistently higher cardiovascular mortality when compared with urban populations (Aggarwal et al., 2021; Liu et al., 2025; Peterson et al., 2023; Chaganty et al., 2023). Evidence indicated slower improvement in cardiovascular outcomes over time within rural communities (Aggarwal et al., 2021; James et al., 2017). Younger adults residing in rural areas increasingly demonstrated high cardiometabolic risk, suggesting early accumulation of disadvantage (Liu et al., 2025). These geographic disparities were closely associated with socioeconomic hardship, food insecurity, housing instability, and reduced access to preventive health resources (Bazoukis et al., 2025; Brandt et al., 2023; American Heart Association, 2023). Home-based cardiac rehabilitation, tele-rehabilitation, and hybrid rehabilitation models have demonstrated encouraging improvements in participation among patients facing transportation and geographic barriers. Expanding insurance coverage for these services may further improve long-term cardiovascular outcomes while reducing disparities in secondary prevention.
Disparities in Early Detection and Screening
The literature revealed marked inequities in the early detection of cardiovascular disease and associated risk factors. Racial and ethnic minority populations were less likely to receive routine preventive assessments for elevated blood pressure, abnormal lipid levels, and impaired glucose regulation (Ali et al., 2024; Benjasirisan et al., 2024). Lower rates of comprehensive cardiovascular risk evaluation were observed even within insured populations in several settings (Lu et al., 2023; Faloye et al., 2024).
Rural populations also demonstrated reduced participation in preventive health services. Limited availability of primary care providers, extended travel distances, and financial constraints were frequently identified as barriers to routine screening and follow-up (Peterson et al., 2023; Lipid Association, 2021–2022; American Heart Association, 2023). These barriers contributed to the delayed identification of cardiovascular risk factors within rural communities (Liu et al., 2025; Chaganty et al., 2023).
Detection and Awareness of Cardiovascular Risk Factors
Disparities extended beyond screening practices to awareness and control of diagnosed conditions. Minority populations with hypertension and dyslipidemia were more likely to remain unaware of their diagnosis and less likely to achieve adequate control following diagnosis (Zakeri et al., 2024; Ali et al., 2024). Similar patterns were observed among rural populations, where undiagnosed and poorly controlled hypertension and diabetes were more common (Liu et al., 2025; Peterson et al., 2023).
Delayed detection resulted in reduced opportunities for early intervention and primary prevention. Delayed detection was associated with presentation at more advanced stages in several settings, with evidence of cumulative organ damage, including structural cardiac changes and subclinical vascular disease (Minhas et al., 2024; Anand et al., 2025).
Disparities in Management and Treatment
Differences in management and treatment were evident across the continuum of cardiovascular care. In the context of primary prevention, racial and ethnic minority populations consistently received less intensive preventive therapy despite meeting established clinical thresholds (Ali et al., 2024; Lu et al., 2023; Faloye et al., 2024). Lower use of lipid-lowering therapy, antihypertensive treatment, and smoking cessation support contributed to poorer control of modifiable risk factors (Lu et al., 2023; Benjasirisan et al., 2024). Differences in treatment initiation, follow-up intensity, and long-term adherence further widened outcome gaps (Faloye et al., 2024).
Rural populations faced additional challenges related to health system capacity. Limited access to specialist services, nutrition counseling, and structured lifestyle interventions hindered effective long-term risk factor management (Peterson et al., 2023; Lipid Association, 2021–2022). These constraints contributed to persistent disparities in blood pressure control, lipid management, and glycemic regulation (Liu et al., 2023; Van Iterson et al., 2023).
Acute Care and Cardiovascular Procedures
Disparities were also evident during acute cardiovascular events. Individuals residing in rural communities experienced a lower likelihood of receiving timely evidence-based diagnostic evaluation and therapeutic intervention during hospitalization (Chaganty et al., 2023; Aggarwal et al., 2021). Minority populations were less likely to receive advanced imaging and invasive management when clinically indicated (Faloye et al., 2024; Houston Methodist DeBakey CV J, 2022). These differences were associated with increased short-term complications and higher mortality (Minhas et al., 2024; Aggarwal et al., 2021).
Secondary Prevention and Cardiac Rehabilitation
Participation in secondary prevention services remained uneven across populations. Engagement in cardiac rehabilitation programs was consistently lower among racial and ethnic minority populations and among rural communities (Liu et al., 2023; Van Iterson et al., 2023). Geographic distance to rehabilitation centers, transportation limitations, employment obligations, and caregiving responsibilities were commonly cited barriers (Van Iterson et al., 2023; American Heart Association, 2023). Reduced participation in rehabilitation limited opportunities for functional recovery and sustained risk factor modification, contributing to persistent disparities in long term cardiovascular outcomes (Liu et al., 2023; Anand et al., 2025).
Social and Structural Determinants of Observed Disparities
Across studies, social and structural determinants emerged as central drivers of cardiovascular inequities. Socioeconomic disadvantage influenced access to preventive services, affordability of medications, and capacity to engage in long term disease management (Bazoukis et al., 2025; Brandt et al., 2023). Neighborhood conditions, including limited access to healthy food options and safe environments for physical activity, further shaped cardiovascular risk (American Heart Association, 2023; NIH/AHA, 2025).
Health system characteristics also played a significant role. Limited availability of culturally responsive care, underrepresentation of minority populations in cardiovascular leadership, and bias within clinical decision-making contributed to differences in treatment intensity and patient communication (Javed et al., 2022; Faloye et al., 2024). Structural underinvestment in rural health systems, including workforce shortages and infrastructure limitations, further amplified observed disparities (Lipid Association, 2021–2022; Health Policy Today, 2025).
Evidence on Strategies to Address Disparities
Although much of the literature focused on documenting disparities, emerging evidence identified several strategies with the potential to reduce inequities. Community-engaged prevention initiatives demonstrated improvements in cardiovascular risk factor control within minority populations (Anand et al., 2025; Brandt et al., 2023). Integrated primary care models incorporating multidisciplinary teams enhanced detection and management in resource-constrained settings (Peterson et al., 2023; Chaganty et al., 2023). Expansion of digital health approaches showed promise in reducing geographic barriers, although effectiveness depended on adequate infrastructure and patient support (NIH/AHA, 2025; Health Policy Today, 2025). Policy initiatives addressing insurance coverage, food security, and health system investment were associated with improved cardiovascular outcomes in selected contexts (American Heart Association, 2023; BIDMC, 2025). Adoption of equity-focused performance measures supported systematic monitoring and accountability within health systems (Brandt et al., 2023; Bazoukis et al., 2025).
The study selection process is illustrated in the PRISMA 2020 flow diagram (Figure 1).
Discussion
Summary of Principal Findings
This systematic review highlights persistent and widespread inequities in cardiovascular disease burden, detection, and management affecting racial and ethnic minority populations and individuals living in rural communities (Minhas et al., 2024; Muncan, 2018; Anand et al., 2025; Aggarwal et al., 2021; Liu et al., 2025). Across diverse settings, these populations experience higher prevalence of cardiovascular risk factors and worse clinical outcomes, while simultaneously facing reduced access to timely detection and evidence-based management (Javed et al., 2022; Nair et al., 2024; Bazoukis et al., 2025). Disparities were observed throughout the continuum of care, beginning with preventive screening and extending through long-term disease management and secondary prevention (Ali et al., 2024; Benjasirisan et al., 2024; Faloye et al., 2024; Van Iterson et al., 2023). These inequities occur across the continuum of care and collectively contribute to sustained differences in cardiovascular morbidity and mortality (Brandt et al., 2023; Anand et al., 2025).
Interaction of Social Identity and Geographic Context
The synthesis underscores the importance of considering social identity together with geographic context in understanding cardiovascular inequities (Javed et al., 2022; Bazoukis et al., 2025). Racial and ethnic minority status and place of residence jointly influence exposure to risk, access to care, and quality of treatment (Minhas et al., 2024; Aggarwal et al., 2021; Liu et al., 2025). Individuals from minority populations residing in rural communities frequently encounter layered disadvantage related to socioeconomic conditions, health system capacity, and structural inequities (James et al., 2017; Brandt et al., 2023).
Urban environments also present distinct challenges. Minority populations concentrated in disadvantaged urban neighborhoods are often exposed to environmental hazards, limited availability of health-promoting resources, and chronic psychosocial stress (Javed et al., 2022; Bazoukis et al., 2025). These factors contribute to early accumulation of cardiovascular risk and earlier disease onset (Minhas et al., 2024; Nair et al., 2024). Effective responses therefore require recognition of how social identity and geographic context interact to shape cardiovascular health (Brandt et al., 2023).
Implications for Clinical Practice
The findings of this review have important implications for clinical care delivery. Health professionals and health systems should prioritize equitable approaches to cardiovascular risk assessment by ensuring consistent screening for blood pressure abnormalities, glycemic dysregulation, and lipid disorders among high-risk populations (Benjasirisan et al., 2024; Ali et al., 2024). Greater emphasis on early identification can reduce delays in diagnosis and improve prevention outcomes (Minhas et al., 2024; Anand et al., 2025).
Management strategies should reflect the elevated risk profiles observed among minority populations and rural communities. More consistent application of guideline-based preventive therapies, combined with close follow-up and support for long term adherence, is essential (Ali et al., 2024; Lu et al., 2023; Faloye et al., 2024). Incorporation of social determinants into routine clinical assessment can help identify barriers that limit treatment effectiveness, including food insecurity, transportation challenges, and financial strain (Bazoukis et al., 2025; Brandt et al., 2023).
Expanding access to cardiac rehabilitation and secondary prevention services is also critical. Community-based delivery models and home-centered approaches may improve participation among populations facing geographic and logistical constraints (Van Iterson et al., 2023; Liu et al., 2023). Collaboration with community organizations and trusted local leaders can enhance cultural relevance and patient engagement (American Heart Association, 2023).
Policy and Health System Considerations
Reducing cardiovascular disparities requires coordinated action beyond the clinical setting. Policies that strengthen health insurance coverage and reduce financial barriers to preventive and chronic care can improve access to essential services (American Heart Association, 2023; Brandt et al., 2023). Investment in rural health infrastructure, including workforce development and digital capacity, is necessary to address long-standing gaps in care availability (Lipid Association, 2021–2022; NIH/AHA, 2025).
Health systems serving minority dense urban communities also require sustained support to ensure adequate resources and high-quality services (Bazoukis et al., 2025; Health Policy Today, 2025). Incorporation of equity-focused performance measures into accountability frameworks can promote systematic monitoring of disparities and encourage targeted improvement efforts (Brandt et al., 2023). Broader policy initiatives addressing housing stability, transportation access, education, and environmental conditions are also central to advancing cardiovascular equity (NIH/AHA, 2025; BIDMC, 2025).
Research Gaps and Future Directions
Despite extensive documentation of disparities, important gaps remain in the evidence base. Few prospective studies have been specifically designed to evaluate interventions aimed at reducing inequities in early cardiovascular detection and management (Anand et al., 2025; Brandt et al., 2023). Variation in definitions of race, ethnicity, and geographic context limits comparability across studies and complicates the synthesis of findings (James et al., 2017; Hutchinson and Shin, 2014).
Several populations remain underrepresented in cardiovascular research, including American Indian populations, Alaska Native populations, migrant communities, and populations in low income and middle-income regions (Hutchinson and Shin, 2014; James et al., 2017). Future investigations should adopt intersectional analytic approaches that account for the combined influence of social identity, socioeconomic position, and geographic context (Javed et al., 2022; Bazoukis et al., 2025). Implementation science methods will be essential to translate effective interventions into scalable and sustainable practice (Anand et al., 2025).
Strengths and Limitations
This review benefits from a comprehensive search strategy spanning multiple databases and the inclusion of recent high-quality evidence (Minhas et al., 2024; Anand et al., 2025). The integrated examination of racial, ethnic, and geographic disparities provides a multidimensional perspective on cardiovascular inequities and highlights shared structural drivers across settings (Brandt et al., 2023).
Several limitations should be acknowledged. Substantial heterogeneity in study design, outcome definitions, and measurement approaches limited the ability to conduct quantitative synthesis (Chaganty et al., 2023; Peterson et al., 2023). Much of the available evidence originates from high-income countries, which may limit applicability to other contexts (Muncan, 2018; Anand et al., 2025). Publication bias and limited reporting of null findings may also influence the observed patterns (Brandt et al., 2023).
Conclusion
This systematic review demonstrates that racial and ethnic minority populations and individuals residing in rural communities experience persistent and systematic disadvantages in the early detection and management of cardiovascular disease (Minhas et al., 2024; Aggarwal et al., 2021; Liu et al., 2025). These inequities span the full continuum of care, beginning with lower rates of preventive screening and delayed diagnosis and extending through reduced access to evidence-based treatment, secondary prevention services, and long-term disease management (Ali et al., 2024; Benjasirisan et al., 2024; Faloye et al., 2024; Van Iterson et al., 2023). The resulting disparities contribute to higher disease burden, worse clinical outcomes, and avoidable premature mortality within these populations (Anand et al., 2025; Bazoukis et al., 2025).
The evidence synthesized in this review indicates that these patterns are not explained by biological differences alone. Instead, they reflect the cumulative effects of social, structural, and health system inequities that shape exposure to risk, access to care, and quality of treatment (Javed et al., 2022; Brandt et al., 2023). Socioeconomic disadvantage, unequal distribution of health-promoting resources, limited health system capacity in rural settings, and persistent structural discrimination collectively create conditions that disadvantage minority populations and rural communities throughout the life course (Bazoukis et al., 2025; NIH/AHA, 2025).
Addressing cardiovascular disparities therefore requires coordinated action across multiple levels. Policy interventions that reduce poverty, strengthen social safety nets, and expand access to affordable health coverage are essential for improving access to preventive and chronic cardiovascular care (American Heart Association, 2023; BIDMC, 2025). Sustained investment in health infrastructure serving rural communities and minority populations is necessary to improve the availability of primary care, specialty services, and secondary prevention programs (Lipid Association, 2021–2022; Health Policy Today, 2025). Within health systems, equity-focused quality improvement efforts that incorporate measurement of disparities and accountability for outcomes are critical for reducing gaps in detection and treatment (Brandt et al., 2023). Community-engaged approaches that deliver culturally responsive and context-specific prevention and care can further enhance trust, engagement, and effectiveness among populations historically underserved by health systems (Anand et al., 2025).
If these strategies are implemented at scale and sustained over time, they hold substantial potential to reduce overall cardiovascular disease burden while also narrowing long-standing inequities in cardiovascular health (Bazoukis et al., 2025; Brandt et al., 2023). Progress toward equitable cardiovascular outcomes will require continued commitment from policymakers, health systems, clinicians, researchers, and communities (American Heart Association, 2023). Advancing equity in cardiovascular prevention and care is not only a public health imperative but also a necessary step toward improving population health and reducing preventable disparities across racial, ethnic, and geographic lines (Anand et al., 2025).
References
- American Heart Association. Health disparities among the many unique challenges for people in rural America. American Heart Association News. 2023.
- Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease. Circulation. 2019;140:e596-e646.
- Churchwell K, Elkind MSV, Benjamin RM, et al. Call to action: Structural racism as a fundamental driver of health disparities. Circulation. 2020;142(24):e454-e468.
- Carnethon MR, Pu J, Howard G, et al. Cardiovascular health in African Americans: A scientific statement from the American Heart Association. Circulation. 2017;136:e393-e423.
- Minhas AMK, et al. Racial and ethnic disparities in cardiovascular disease. Curr Opin Cardiol. 2024.
- Muncan B. Cardiovascular disease in racial/ethnic minority populations: a review. Public Health Rev. 2018;39:32.
- Javed Z, et al. Race, racism, and cardiovascular health: applying a structural approach. Circ Cardiovasc Qual Outcomes. 2022;15(2):e007917.
- Nair L, et al. Ethnic disparities in risk factors, morbidity, and mortality of cardiovascular disease. J Endocr Soc. 2024;8(7):bvae116.
- Anand SS, et al. Reducing inequalities in cardiovascular disease: focus on ethnic disparities. Lancet Reg Health Eur. 2025.
- Aggarwal R, et al. Rural–urban disparities: diabetes, hypertension, heart disease, and stroke mortality among Black and White adults, 1999–2018. J Am Coll Cardiol. 2021;77:11-20.
- Liu M, et al. Cardiovascular health among rural and urban US adults. JAMA Cardiol. 2025.
- Peterson L, et al. Disparities in screening, prevention, and management of cardiovascular disease in rural populations. Curr Atheroscler Rep. 2023;25(10):627-639.
- Hutchinson RN, Shin S. Systematic review of health disparities for cardiovascular disease and diabetes in American Indian and Alaska Native populations. PLoS One. 2014;9(1):e80973.
- James CV, et al. Racial/ethnic health disparities among rural adults—United States, 2012–2015. MMWR Surveill Summ. 2017;66(23):1-9.
- Taylor HA, et al. Cardiovascular disease among women residing in rural areas. Am J Public Health. 2002;92(4):548-551.
- Chaganty SS, et al. Rural and urban disparities in cardiovascular disease–related mortality in the United States. Heart Lung Circ. 2023.
- Liu Y, et al. Rural–urban disparities in cardiac rehabilitation eligibility and use. JAMA Cardiol. 2023;8(2):157-167.
- Ali MR, et al. Racial and ethnic disparities in primary prevention of cardiovascular disease. Can J Cardiol. 2024.
- Lu Y, et al. National trends in racial and ethnic disparities in use of lipid-lowering medications. JAMA Netw Open. 2023;6(11):e2340225.
- Benjasirisan C, et al. Disparities in the use of annual heart health screenings and cardiovascular risk assessment. J Am Heart Assoc. 2024;13(4):e032919.
- Zakeri M, et al. Racial and ethnic disparities in perceived health status among adults with cardiovascular disease. Prev Chronic Dis. 2024;21:E121.
- Faloye AO, et al. Racial and ethnic disparities in cardiovascular care. J Cardiothorac Vasc Anesth. 2024.
- Bazoukis G, et al. Impact of social determinants of health on cardiovascular outcomes. J Am Heart Assoc. 2025;14:e039031.
- Brandt EJ, et al. Assessing and addressing social determinants of cardiovascular health. J Am Coll Cardiol. 2023;81(11):1037-1053.
- Van Iterson EH, et al. Geographical and urban–rural disparities in cardiac rehabilitation use. JAMA Cardiol. 2023;8(2):168-178.
- Lipid Association. Cardiovascular disease in the rural American population. LipidSpin. Winter 2021–2022.
- AHA Newsroom. Health disparities among the many unique challenges for people in rural America. American Heart Association; 2023.
- NIH / AHA report. Social factors explain poorer cardiovascular health in rural areas. 2025.
- BIDMC. Rural Americans have higher rates of heart disease, study finds. 2025.
- Health Policy Today. Rural and racial gaps in heart health. 2025.
- Hutchinson RN, et al. Health disparities for AI/AN populations: CVD and risk factors. PLoS One. 2014;9(1):e80973.
- Houston Methodist DeBakey CV J. Population-level gaps in coronary artery disease care. 2022.
- Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration. BMJ. 2021;372:n160.
- Thomas J, Harden A. Methods for thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8:45.
- Popay J, Roberts H, Sowden A, et al. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews. ESRC Methods Programme; 2006.
- Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics—2024 update: A report from the American Heart Association. Circulation. 2024;149:e347-e913.
- Van Iterson EH, et al. Geographical and Urban–Rural Disparities in Cardiac Rehabilitation Utilization. JAMA Cardiol. 2023;8(2):168-178.